

Introduction:
Indolent T-cell lymphoproliferative disorder of the gastrointestinal tract (ITCLD-GT) is a newly recognized entity in the 2016 revision of the World Health Organization (WHO) classification of lymphoid neoplasms. ITCLD-GT is defined as a clonal T-cell proliferation occurring in the GT, mostly in colon and small bowel. So far only 52 ITCLD-GT cases have been reported. It has a pathologically nondestructive expansionary growth pattern, a less than 10% Ki67 proliferative index and an indolent clinical course. However, the pathological characteristics of ITCLD-GT in lesions except the small and large intestines, its clinical progress/transformation and pathogenetic mechanisms and molecular alterations remain unknown.
Methods:
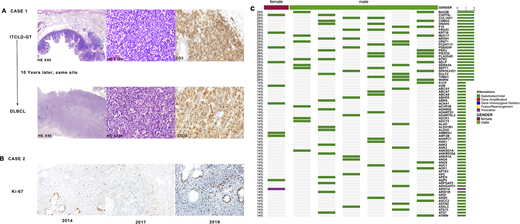
Nine ITCLD-GT cases were collected from one center in southwest China, and their clinicopathological were analyzed. Of these patients, 7 had indolent clinical courses; one had lymph node metastasis in the late stage; and another one transformed into diffuse large B-cell lymphoma (DLBCL) after 16 months (Figure A). In one patient, neoplastic cells involved most of the digestive tract from esophagus to rectum. Whole-exome sequencing was performed in 9 samples from 7 cases. Genome-wide mutation landscape was analysed on these ITCLD-GT samples and pairwise comparison was made between stomach and colon lesions as well as between ITCLD-GT and transformed DLBCL samples. Gene Ontology (GO) enrichment and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway analysis were performed.
Results:
The median age of the patients was 47 years, and the male/female ratio was 7:2. Clinically, these patients presented with diarrhea with or without abdominal pain, abdominal distension, fatigue or hematochezia. Colonoscopy showed thickened intestinal mucosa in 8 cases, with small nodularity and folds in 7 cases and polyps resembling in 1 case. Intestinal mucosa surfaces showed patchy erythema, erosion or superficial ulcer with diameter ≥ 2.5cm. Endoscopy showed thickened gastric mucosa, nodular protrusion or multiple wide pedicle polyps. Microscopically, the lamina propria was displaced by the infiltrate of dense, monotonous and small lymphocytes, but the mucosal glands were not destroyed. All the infiltrated lymphocytes were positive for CD3p and TIA-1, mostly positive for CD2, CD5 and CD7 and negative for CD20 and Granzyme B. 8 cases were positive for CD8 and 1 case expressed CD4. In the case with esophagus and GT involvement, CD56 was positive in gastric and intestinal lesions, but negative in esophageal and colon. The proliferative index of Ki67 was less than 10% in all cases at diagnosis, but in one case it increased to 20% after 4 years (Figure B). In all cases, monoclonal TCR gene rearrangement was positive and EBER1/2 was negative.
The landscape of gene alterations using WES in these patients were analysed (Figure C). The recurrent mutated genes included cancer-related gene PDE4DIP, transcription regulatory genes BAZ2B and CNOT6L, signaling transduction-related genes MUC17 and PIEZO2, metabolism regulatory genes PLA2G4D and FRG2C, cytoskeleton and cell adhesion-associated genes COL14A1, DNAH5 and many other genes were shown in Figure C. GO analysis showed that mutated genes were significantly enriched in microtubule cytoskeleton organization. KEGG pathway analysis indicated that the mutated genes were mostly enriched in focal adhesion and ECM-receptor interaction, both associated with cancer development. Pairwise comparison analysis of lesions from the stomach and colon showed that there was almost no genetic difference between the two lesions. JAK3, NRAS and SETD2 mutations and BCOR deletion may contribute to the entire digestive tract distribution of ITCLD-GT. The transformed aggressive DLBCL sample carried 253 more mutated genes than the indolent ITCLD-GT sample. Mutations of TP53, ARID1A, KMT2D and M2P2K1 only in the DLBCL sample may contribute to the transformation of ITCLD-GT to DLBCL.
Conclusion:
Our study summarized the clinicopathological characterization of 9 cases of ITCLD-GT. ITCLD-GT is generally inert, but it may develop with an increased Ki67 proliferation index in the late stage or even turn into aggressive DLBCL. We characterized the genomic alterations in ITCLD-GT and revealed its molecular pathogenesis and progression, which might be helpful for diagnosis, prognosis and treatment of this rare lymphoid neoplasm.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal